
As a physical therapist, I encounter quite many people with shoulder pain or issues. When it comes to no trauma or age-related issues there is one most common reason for shoulder pain. That reason is Shoulder impingement syndrome or shoulder tendonitis.
Now, what is shoulder impingement syndrome, or SIS?
Well simply put it’s the continuous excess rubbing and compression of rotator cuff muscle tendons. As those tendons are extremely close to each other, the excess rubbing leads to inflammation and swelling. The swelling causes the space where those tendons sit too narrow, leading to more irritation and pain. This reduces your ability to move your arm from your shoulder.
Anatomy and Function of rotator cuff
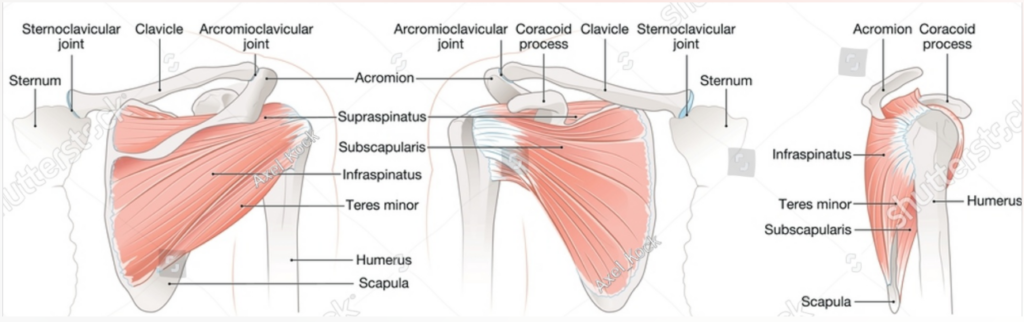
Rotator cuff consists of 4 muscles: supraspinatus, infraspinatus, subscapularis and teres minor.
The function of the mentioned muscles is abduction, which means to laterally raise the arm from the side of the body upwards, as well as internal and external rotation.
All of those muscles have insertion on the top of the bone called the humerus, bone of the upper arm. They as well pass underneath the acromion, which is the tip of the outer edge of a shoulder blade. Acromion meets clavicula, your collar bone, at the very end also.
This makes the passage through which muscle tendons have to pass by quite tight and narrow.
What are the symptoms of shoulder impingement syndrome?
As the muscles of the rotator cuff have many different functions, that leads to the development of many symptoms.
Note that not all muscles have to be inflamed nor that you need to have all of the symptoms to have shoulder impingement syndrome. You can develop inflammation in only one muscle and have a few of the symptoms as well.
That is why it’s important to consult and get examined by a licensed physical therapist.
The symptoms are the following:
- Raising the arm above the head level causes pain,
- Difficulties or pain when lowering your arm from a raised position,
- Warmth, tenderness, or pain in the front side of the shoulder,
- Lying on the shoulder is painful, may lead to difficulties sleeping,
- Reaching behind or to the different sides of the body is painful,
- Weakness and stiffness
How does shoulder impingement syndrome develop?
As mentioned above the tendons of muscles from the rotator cuff is inserted in a very narrow space between the bone of the upper arm and the edge of the shoulder blade.
Certain arm movements cause compression of those tendons. Usually, it is an overhead arm movement or bad posture that leads to compression.
When performed repeatedly for prolonged periods of time it causes irritation and inflammation to the tendons and area. Eventually, the internally swollen area leads to decreased mobility, stability, and pain.
Unfortunately because of the anatomy of the area the swelling and irritation increase over time. The further narrowing of space if left untreated will lead to worse mobility and increased pain.
This is most common amongst athletes such as basketball, volleyball, baseball players, weightlifters, and manual laborers.
Almost every occupation where workers’ movement of the arm is performed in the stretched and flexed position is at risk. Even older adults can develop shoulder impingement as it can be caused by wear and tear.
How to treat?
First and foremost you need to rest and ice the shoulder. In some cases even take anti-inflammatory medicine. This is something that many will do and in most cases, the pain will decrease.
Unfortunately, the pain usually comes back. This happens because of the fact that the issue wasn’t combated at its core.
In most cases, there is a need for personal reflection about how you can change your working stance and regime.
We refer to this as ergonomy. Changing your working ergonomy is the actual first step you can take towards dealing with shoulder impingement syndrome long term. Try switching the working stance often, if possible incorporate more short breaks.
Now the other important thing that you want to do is contact a physical therapist for an accession. The aspects that will be treated are mobility, strength, stability and transition back to functional activities.

Mobility Training
In many cases, mobility is the main limiting factor when it comes to shoulder impingement.
Mobilization of the shoulder joint comes from a range of motion exercises and manual therapy. Range of motion exercises consist of a variety of different stretches and exploring the painful movements in a safe manner.
Those movements and stretches are performed by different techniques which you go through with your physical therapist. I will be going through them with you in a post to come.
Manual therapy consists of physical therapists releasing pressure from and mobilizing your joints and muscles hand on. Some of the hands-on work may be discomforting as the pressure points are being released.
The advantage of manual therapy is that you do not actively have to contribute and it primes your mobility for further training. Releasing the trigger points, spots around your shoulder blade that hurt the most, can be in some cases done by yourself.
Even the mobilization of surrounding muscles such as lats can further increase mobility. For you to be able to do that yourself you would need a foam roller, massage ball or massage gun.
Stability Training
One of the most underlooked aspects in the rehabilitation of shoulder impingement syndrome or general shoulder pain is stability.
Rotator cuffs’ actual main function is to keep the shoulder stable throughout the movement.
Training stability is often overlooked in my opinion as we treat impingement syndrome as purely muscle weakness. The weakness in a muscle comes from the inflammation of the insertion point of the muscle, or to be more precise tendons.
As mentioned at the beginning of the post it is the tendons of the shoulder blades muscles that insert on the humerus head. To train your tendons or lower the inflammation in them, a certain kind of training has been shown to be beneficial.
Those training forms are eccentric and isometric.
Eccentric means the stretching or lowering part of the movement. Isometric means that you hold your muscle under constant tension. Throughout my research and experience, I find that integrating those two training forms is game-changing for your shoulder health.
Strength Training
Because of the lack of movement caused by pain and ongoing swelling the affected muscles become weak.
That leads to imbalances not only in your shoulder but the body as a whole. Those imbalances and weaknesses need to be addressed.
Depending on what your individual “injury” looks like, a physical therapist will design a personalized plan for you. The plan will be safe and progress over time. The areas of pain and weakness will be addressed by performing resistance training.
Usually, at the beginning the exercises will be combined with the mobility treatment, ensuring the appropriate progression to more difficult ones. Mobility exercises may consist of work from table and bed, later performing more advanced ones with equipment and machines.
Functional training
Functional training consists of performing activities and movements that you usually do in your everyday life or work.
Those activities may be just the ones that led to shoulder impingement.
That is why teaching your body how to adapt, perform safe and controlled movements is necessary. This sort of training is performed at the end of the rehabilitation period. By that time the majority of the pain and mobility restrictions, if not all, have subsided.
The training will mostly be oriented around your goals in consultation with a physical therapist. As you achieve your goals the rehabilitation ends.